

Abstract
Introduction: The source of chimeric antigen receptor (CAR) T cells can be autologous or allogeneic, depending on the history of allogeneic hematopoietic stem cell transplantation (allo-HSCT). For patients with a history of allo-HSCT, CAR T cells are allogeneic, which can be manufactured from donors' peripheral blood mononuclear cells (PBMC) (donor-derived allogeneic CAR T cells, DD-alloCAR) or patients' own PBMC (recipient-derived allogeneic CAR T cells, RD-alloCAR). Unlike autoCAR T cells, which are activated by CAR only, alloCAR T cells receive activation signals from both T-cell receptor and CAR. The difference could affect CAR T-cell biology, resulting in different clinical outcomes.
Methods: We retrospectively reviewed 31 consecutive patients who received CAR T-cell therapy in our center. Patients were divided into three groups, as autoCAR group, DD-alloCAR group and RD-alloCAR group. We compared the efficacy and safety profiles among the three groups. We also performed a subgroup analysis of patients received alloCAR.
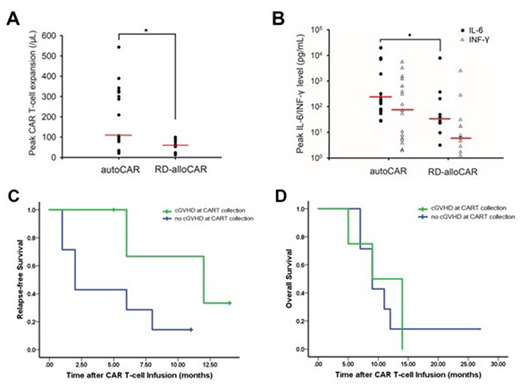
Results: Altogether there were 17 patients in the autoCAR, 11 in the RD-alloCAR and 3 in the DD-alloCAR groups. After a median follow-up of 9 months, the CR rate was 88.2% (95% CI 63.6-98.5%) in the autoCAR group and 100% (95% CI 71.5-100%) in the RD-alloCAR group, which had no significant difference (p=0.73). CR rate in DD-alloCAR was 66.7% (95% CI 9.43-99.1%). The median peak expansion of CAR T cells in the autoCAR was significantly higher than the RD-alloCAR group (p=0.007, Figure A). However, the median OS and EFS did not differ significantly among the groups. As far as adverse effects, RD-alloCAR group had significantly less patients with severe CRS (defined as Grade ≥ 3) than the autoCAR group (p=0.049), with significantly lower peak IL-6 level (p=0.021, Figure B). Neurotoxicity and the degree of cytopenia did not have significant difference among the groups. Acute GVHD occurred in 2 (18.2%) RD-alloCAR patients and 1 (33.3%) DD-alloCAR patients following CAR T-cell infusion. Univariate subgroup analysis of the patients who received alloCAR T-cell therapy showed the presence of cGVHD at the time of PBMC collection was significantly associated with less 6-month relapses (p=0.022); the median RFS in the no-cGVHD group was 2.00 (95% CI 0.72 to 3.28) months, compared to 12.0 (95% CI 2.40 to 21.6) months in the cGVHD group (p=0.084, Figure C); the median OS had no significant difference (Figure D). RD-alloCAR patients with or without cGVHD at PBMC collection did not differ in terms of the peak CAR T-cell expansion, CRS grades or OS.
Conclusions: Compared with autoCAR, RD-alloCAR had similar efficacy but less severe CRS. For RD-alloCAR T-cell therapy, the presence of cGVHD at the time of PBMC collection was associated with fewer 6-month relapses. DD-alloCAR and RD-alloCAR T-cell therapies were effective and safe without causing significant GVHD.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal